
Do COVID-19 Vent Protocols Need a Second Look? – Dr. Kyle Sidell Expresses Concern (Excellent video)
Here’s another from April 14th (short):
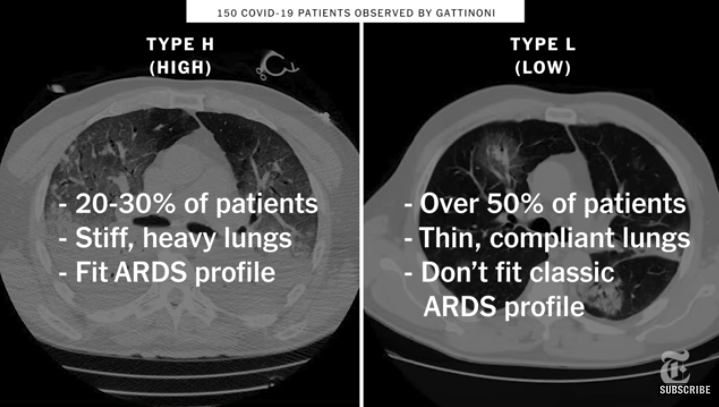
If you don’t know what type you are dealing with (according to researcher Gattinoni): “it can result in disaster for 50% of the [treatment] population.”
Dr. Cameron Kyle Sidell. E R & Critical Care Dr From NYC:
Dr. Kyle Sidell Expresses Concern That We Might Not Be Treating COVID 19 But A Totally Different Medical Phenomenon & We Should Do Something About It.
https://www.medscape.com/viewarticle/928156?scr=soc_yt_200311_mscpedt_news_mdspc_COVIDJOHN&faf=1
HELPFUL HINT: If you want a medication/regimen to be given (hydroxychloroquine, IV Vitamin C, zinc, etc) you have to report it as an “at-home medication” in order for them to do so and demand that it be continued (a tip from inside the system).
Death rate after being put on ventilators is anywhere from 30% to 90%….70% reported average. Intubation for a ventilator, according to newer data, should be a last resort after focusing more on actual oxygenation, rather than mere “breathing assistance”.
An additional consideration not mentioned in these videos involves vested financial incentives driving diagnosis and treatment approaches.
According to a MN State Senator, Dr. Scott Jensen), Medicare includes a $13,000 payment for each COVID-19 diagnosed admission, And a $39,000 benefit to the hospital if the patient goes onto a ventilator. [See news video: https://youtu.be/PV_a1u7mq3g]
Conversely, a Medicare patient who is diagnosed with a simple, garden variety non-COVID related pneumonia (which is by far more common) allows a hospital to receive a one time Medicare lump sum payment of merely $4,600. But if they diagnose COVID-19 related pneumonia, they get just under three times that amount. Ka-CHING!
Call me crazy, but do you think it sounds as though there might just be some added incentive there?
Also, there is a very high mortality rate associated with persons going on a ventilator (an average of 70% mortality rate), for a variety of reasons. It is not necessarily a benign intervention. For one thing, patients on ventilators run a higher risk of developing pneumonia because of frequently antibiotic resistant bacteria that can enter through the breathing tube. It’s a very dangerous significant risk factor for anyone going on a ventilator. The ventilator can also make it difficult for them to cough and clear airways of irritants that can cause infections.
One of the motivations behind their widespread use is the fact that they create a closed ventilation loop, thereby supposedly limiting the spread of germs through normal breathing into the collective environment. But that closed ventilation loop also has the potential to amplify the effects other pathogens (bacteria and other viruses) in the patient. This is why they are all so pumped full of antibiotics—useless against viruses– at the same time. As you may already logically realize, antibiotics may not help when it comes to the presence antibiotic-resistant bacteria, and definitely does not help when it comes to shoring up any person’s innate immunity or the health of anyone’s all-important microbiome. Antibiotics ultimately make and immune system more vulnerable in the long run, and not less.
Furthermore, New York ER doctor, Cameron Kyle-Sidell [https://www.youtube.com/watch?v=sKExxcD26_I], has made public statements about the misuse of ventilators with supposed COVID-19 patients. He’s stated that many of these patients actually have functioning lungs. Their more immediate and dire life-threatening situation is straight oxygen deficit, as if they have high-altitude sickness. But pressure on the lungs, applied by the use of ventilators via standard rigid protocols, he says, can cause pulmonary damage, and even death.
Pulitzer prize-nominated journalist, Jon Rappoport decided to follow up on the public remarks stated by Minnesota state senator, Dr. Scott Jensen. He arranged for a private interview, after which he posted the following blog post:
A state senator has suddenly come out of nowhere and made big news.
My conversation with Minnesota State Senator, Dr. Scott Jensen, took place after I read the explosive statement he made to FOX News, on April 9th. So let’s start with his earlier FOX statement:
“Right now Medicare has determined that if you have a COVID-19 admission to the hospital you’ll get paid $13,000. If that COVID-19 patient goes on a ventilator, you get $39,000; three times as much. Nobody can tell me, after 35 years in the world of medicine, that sometimes those kinds of things [don’t] [have] impact on what we do…”
I reached out to Senator Jensen, and obtained clarification. Jensen told me his remark pertained to patients with Medicare coverage. And the 2 payouts he mentioned are standard insurance payments from Medicare which would go to the hospital.
Of course, he explained, some hospitals have a pay-share plan with their staff doctors. Therefore, a windfall for the hospital is passed along to those doctors.
Jensen told me: Take a Medicare patient who is diagnosed with simple non-COVID pneumonia. The hospital would receive a one-time Medicare lump-sum payout of $4600.
However, if that Medicare patient is diagnosed with COVID-19 pneumonia, the Medicare coverage is a one-time $13,000 payment. And if the hospital puts that COVID-19 pneumonia patient on a ventilator, the one-time payment is $39,000. NOTE: It doesn’t matter how long these patients stay in hospital—there is only going to be one lump-sum insurance payment.
So, I infer, there are several types of financial incentives for hospitals:
1) Diagnose as many people as possible with COVID-19.
2) Diagnose as many people as possible with COVID-19 who have light symptoms–making it easy to move them out of the hospital quickly.
3) Put as many COVID patients as possible on ventilators for as short a time as possible.
Under the heading of “diagnose as many patients as possible with COVID-19,” there is also the key question of what constitutes “a COVID-19 patient”—and how the use of that label can be multiplied and manipulated. Senator Jensen made a few choice comments to FOX on this subject as well.
From FOX News: “Dr. Scott Jensen, a Minnesota family physician who is also a Republican state senator, told ‘The Ingraham Angle’ Wednesday that the Centers for Disease Control and Prevention’s (CDC) guidelines for doctors to certify whether a patient has died of coronavirus are ‘ridiculous’ and could be misleading the public.”
“Host Laura Ingraham read Jensen the [CDC] guidelines, which say: ‘In cases where a definite diagnosis of COVID cannot be made but is suspected or likely (e.g. the circumstances are compelling with a reasonable degree of certainty) it is acceptable to report COVID-19 on a death certificate as ‘probable’ or ‘presumed.'”
“In response, Jensen told Ingraham the CDC’s death certificate manual tells physicians to focus on ‘precision and specificity,’ but the coronavirus death certification guidance runs completely counter to that axiom.”
“‘The idea that we are going to allow people to massage and sort of game the numbers is a real issue because we are going to undermine the [public] trust,’ he said. ‘And right now as we see politicians doing things that aren’t necessarily motivated on fact and science, their trust in politicians is already wearing thin’.”
“…Jensen then told Ingraham that under the CDC guidelines, a patient who died after being hit by a bus and tested positive for coronavirus would be listed as having presumed to have died from the virus regardless of whatever damage was caused by the bus.”
“…Jensen also reacted to Dr. Anthony Fauci’s response to a question about the potential for the number of coronavirus deaths being ‘padded,’ in which the NIAID director described the prevalence of ‘conspiracy theories’ during ‘challenging’ times in public health.”
“‘I would remind him that anytime health care intersects with dollars it gets awkward,’ Jensen said.”
Here is where everything Scott Jensen is saying can turn very grim:
As I’ve reported, New York ER doctor, Cameron Kyle-Sidell, has made public statements about the misuse of ventilators with supposed COVID-19 patients. He’s stated that some of these patients actually have functioning lungs. Their immediate and dire life-threatening situation is straight oxygen deficit, as if they have high-altitude sickness. But pressure on the lungs, applied by the use of ventilators via standard rigid protocols, he says, can cause damage, and even death.
Imagine what would happen if another way—NOT ventilators—was found to usefully and safely deliver oxygen to these patients.
The hospitals wouldn’t get their huge $39,000 payout for each Medicare patient put on a ventilator.
What do you think a hospital would say…what decision would the hospital make…would the hospital allow a better and safer and necessary delivery system for oxygen? For every labeled “COVID-19 patient” whose desperate emergency is a straight deficit of oxygen?
Would the hospital forego all those huge Medicare coverage payouts?
For links to Jon Rappoport’s references, see this article on Jon’s blog: https://blog.nomorefakenews.com/2020/04/12/state-senator-and-doctor-exposes-medicare-payouts-for-covid-19-patients/
NOTE: If you know of anyone who is on a ventilator, please read the following articles:
> Important Consideration Regarding Ventilators and Nutrition
> Prone Position in Severe Acute Respiratory Distress Syndrome
> Might Enzymes Help Blood Clotting Associated With COVID-19?
Viable, successful protocols have been developed to treat persons diagnosed with this condition—even those that are elderly and otherwise vulnerable. Naturally, you’ll never hear about this on the mainstream news. But if you or someone you love becomes a victim of this diagnosis (and I’m not necessarily referring to the virus), you need to know that there are highly effective, non-toxic treatments that have nothing to do with being put on a ventilator, jabbed with some experimental biological agent, or treated with toxic experimental drugs.
https://articles.mercola.com/sites/articles/archive/2020/05/29/dr-paul-marik-critical-care.aspx
A nurse Erin Marie Olszewski reveals that at Elmhurst Hospital, non-Covid patients and Covid confirmed patients are housed in the same rooms. People who have tested negative for COVID-19 several times are referred to as “Covid confirmed” and then connected to a ventilator. Respirators are probably the most common cause of death in the pandemic. Tranquilizers and paralytics in combination with a pressure injury kill 90 percent of the people who are ventilated in Elmhurst (and thus in large parts of the world). Nosocomial (hospital-acquired) infections are the main transmission vector.
Correction: the nurse said that her hospital received $29,000 per person with COVID. In truth it’s $13,000 per person, then the hospital receives another $39,000 per person they place on on a ventilator.
___________________________________________________
A brand new published clinical study:
A Novel Approach to Treating COVID-19 Using Nutrition and Oxidative Therapies
Abstract
Objective: This report is a case series of consecutive patients diagnosed with COVID-19 treated with a nutritional and oxidative medical approach. We describe the treatment program and report the response of the 107 COVID-19 patients.
Study Design: Observational case series consecutive.
Setting: A family practice office in a suburb of Detroit, Michigan.
Patients: All patients seen in the office from February through May 2020 diagnosed with COVID-19 were included in the study. COVID-19 was either diagnosed via PCR or antibody
testing as well as those not tested diagnosed via symptomology.
Interventions: Oral Vitamins A, C, D, and iodine were given to 107 subjects (99%). Intravenous solutions of hydrogen peroxide and Vitamin C were given to 32 (30%) and 37 (35%) subjects. Thirty-seven (35%) of the cohort was treated with intramuscular ozone. A dilute, nebulized hydrogen peroxide/ saline mixture, with Lugol’s iodine, was used by 91 (85%).
Main Outcome Measures: History and physical exam were reviewed for COVID-19 symptoms including cough, fever, shortness of breath, and gastrointestinal complaints. Laboratory reports were examined for SARS-CoV-2 results. Symptomatic improvement after treatment was reported for each patient consisting of first improvement, mostly better, and completely better.
Results: There were a total of 107 patients diagnosed with COVID-19. Thirty-four were tested for SARS-CoV-2(32%) and twenty-seven (25%) tested positive. Three were hospitalized (3%) with two of the three hospitalized before instituting treatment and only one requiring hospitalization after beginning treatment. There were no deaths. The most common symptoms in the cohort were fever (81%), shortness of breath (68%), URI which included cough (69%), and gastrointestinal distress symptoms (27%). For the entire cohort, first improvement was noted in 2.4 days. The cohort reported symptoms mostly better after 4.4 days and completely better 6.9 days after starting the program. For the SARS-CoV-2 test positive patients, fever was present in 25 (93%), shortness of breath in 20 (74%) and upper respiratory symptoms including cough in 21 (78%) while gastrointestinal symptoms were present in 9 (33%). The time to improvement in the SARS-CoV-2 test positive group was slightly longer than the entire cohort.
Conclusion: At present, there is no published cure, treatment, or preventive for COVID-19 except for a recent report on dexamethasone for seriously ill patients. A novel treatment program combining nutritional and oxidative therapies was shown to successfully treat the signs and symptoms of 100% of 107 patients diagnosed with COVID-19.
Each patient was treated with an individualized plan consisting of a combination of oral, IV, IM, and nebulized nutritional and oxidative therapies which resulted in zero deaths and recovery from COVID-19.
Newly Published in 2020:
Science, Public Health Policy, and The Law Volume 2:4-22 July, 2020 Clinical and Translational Research
This study helps to confirm much of what I researched and wrote about in my COVID-19 Report. It’s always nice to have strong, scientific AND clinical research verification.
~Nora
PS. If you would like to make a donation to help support my work, you can click the button below. Thank you so much for your support!
![]()
0 Comments